MHI Elite · Men's Health · Testosterone Optimization
Your testosterone didn't just drop. Your system did.
Most TRT clinics ask one question: Is your testosterone low enough to prescribe? At MHI, we ask a better one: Why is your system underperforming — and what is the data actually telling us?
Testosterone is not just about sex drive or muscle. It is a command signal — for energy, drive, mood, metabolism, recovery, cognition, and long-term resilience. When that signal drops, or when it is misread, most men do not collapse. They fade. Slowly. Quietly. Until the person they used to be feels like a different version of themselves.
We have reviewed tens of thousands of labs. We have watched men in their 30s walk in with hormonal profiles that belong to men in their 70s. We have handed results back to patients who were told everything was normal — and explained why that was the wrong standard to use. Normal is not a target. It is a population average. And right now, that average is declining — not just with age, but across generations. A man today is not hormonally comparable to a man in 1980. He is starting from a lower baseline than the men who came before him. Most clinics are not measuring for that reality.
Testosterone was feared for decades. The science has caught up.
For years, testosterone was treated like a dangerous shortcut — something to avoid unless a man was practically falling apart. That fear was built on old assumptions, flawed studies, and a medical culture trained to fear restoration rather than understand it.
A 1941 paper based on three patients — all with late-stage metastatic cancer — became the foundation for decades of clinical caution. That conclusion was never rigorously challenged. It simply became doctrine.
In 2016, Mayo Clinic and Harvard convened a global consensus — 26 institutions, 17 countries, four medical specialties. The conclusion: testosterone does not cause prostate cancer. Testosterone deficiency is a global public health concern and having a deficiency is a legitimate, underdiagnosed medical condition. Therapy, when properly prescribed and monitored, is evidence-based and clinically rational.
In 2023, the TRAVERSE trial — the largest randomized testosterone safety study ever conducted — found no increased risk of heart attack, stroke, or cardiovascular death. In 2024 and 2025, the FDA formally revised its position based on that evidence.
This is not a trend. This is a scientific correction. And it changes the entire conversation about who should be treated, and how.
This is not normal aging. It is a generational shift.
Testosterone levels are not just declining with age — they are declining across generations. A 40-year-old man today is not hormonally comparable to a 40-year-old in 1980. He is operating from a fundamentally different physiological starting point.
Longitudinal research showed a steady 1% per year population-level decline in testosterone, even after adjusting for age, weight, and health status. A landmark meta-analysis of over 43,000 men showed greater than 58% decline in sperm counts between 1973 and 2011 — with the rate accelerating, not stabilizing.
In clinical practice, this shows up unmistakably. After reviewing tens of thousands of labs, it is now uncommon to see men in their 30s with total testosterone above 500 ng/dL without intervention. What was once the norm is now the exception.
The reference ranges used today were built from a population that was already declining. When someone is told they are ‘within normal range,’ what that often means is they look like everyone else who is also struggling.
The environment is driving this. Endocrine-disrupting chemicals, plastics, pesticides, forever chemicals, chronic stress, artificial light, and processed food are not fringe concerns — they are daily inputs that directly affect hormone production.
Your labs can say normal. Your body can still be off.
Lab reference ranges were not designed to reflect ideal human physiology. They reflect the statistical distribution of whoever walked into a lab. That is a population average — not a performance benchmark.
Men with testosterone in the 300 to 500 ng/dL range are routinely told they are fine. But many of these men present with every clinical symptom of deficiency. Total testosterone is only part of the picture. Free testosterone — the fraction the body can actually use — is often low even when total levels appear acceptable.
You can have a total testosterone of 500 and still be functionally deficient. What matters is not the number alone. It is what the system is doing with it.
Most clinics run a single lab panel, compare it to a reference range built from a declining population, and call it a day. At MHI, we look at the full hormonal axis — not just the output, but the system that produces it.
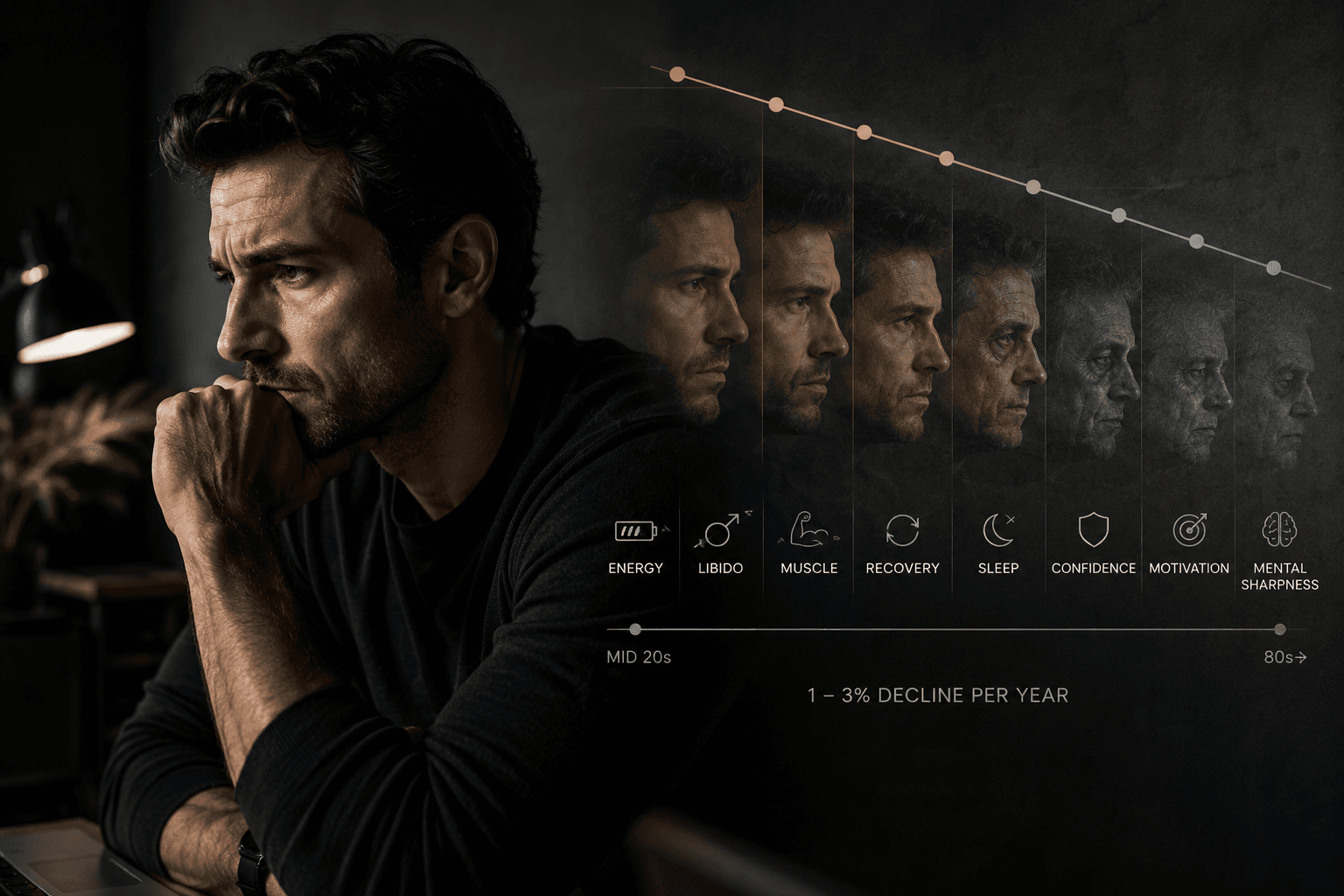
Andropause is quiet. That does not make it harmless.
There is no announcement. No clear event. No dramatic cliff. Just a slow erosion of energy, libido, muscle, recovery, sleep, confidence, motivation, and mental sharpness — starting as early as the mid-twenties, at roughly one to three percent per year.
Because it happens gradually, most men explain it away.
“I'm just busy.” “I'm getting older.” “This is just stress.” “This is normal.” “I just need better sleep.” “I need to train harder.” “I need to cut back on alcohol.” “I'll feel better after this project is done.” “This is normal.”
Maybe. But normal and optimal are not the same thing. The decline is slow enough that the system adapts to dysfunction before the man even recognizes it. By the time it becomes undeniable, it feels like aging — when in reality, it is a measurable, addressable biological shift.
At MHI, we do not call that destiny. We call it a signal.
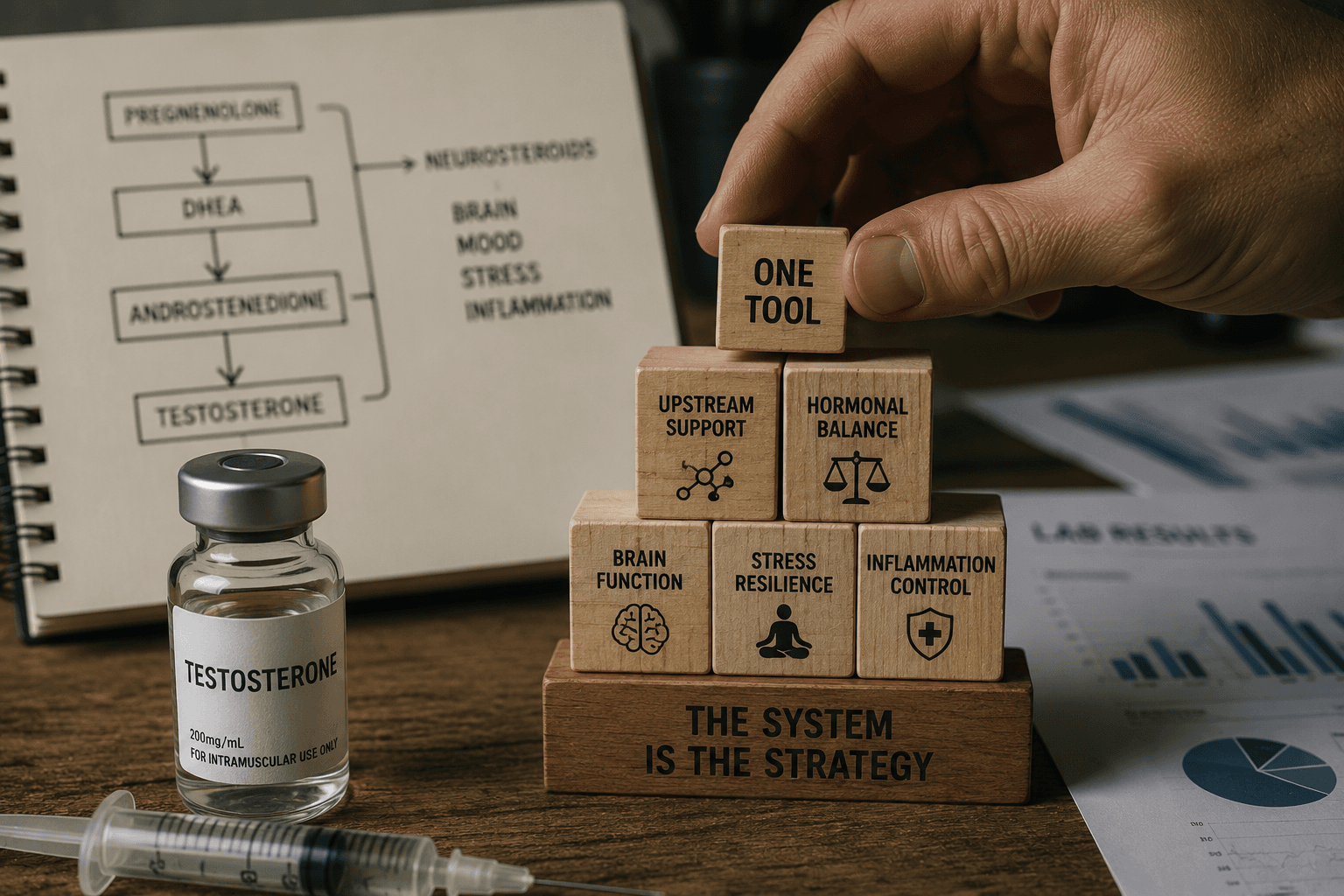
TRT is one tool. The system is the strategy.
Testosterone replacement therapy can be powerful when it is appropriate. But testosterone by itself is not a strategy. It is one instrument inside a much larger system — and introducing it without understanding that system is where most protocols fall short.
Most clinics treat TRT as a simple replacement equation: levels go down, hormone goes in, problem solved. But when testosterone is introduced externally, the body interprets it as sufficiency and begins shutting down internal production. That shutdown does not happen in isolation.
Testosterone sits near the end of a hormonal cascade that begins upstream with compounds like pregnenolone and DHEA — precursors that feed neurosteroid production, brain function, stress resilience, and inflammation regulation. When the axis is suppressed without addressing those upstream elements, patients can reach optimized testosterone levels on paper while still experiencing brain fog, emotional flatness, and poor stress tolerance.
Giving testosterone without understanding the terrain is like injecting capital into a business without reading the financials first. You are not fixing the problem. You are funding it.
At MHI, we do not prescribe testosterone and move on. We evaluate the full hormonal axis. We assess upstream precursors. We build protocols that support the system as a whole — not just optimize a single number.
Not all TRT protocols are the same. Delivery method is not a detail.
Most clinics pick a delivery method based on convenience or cost. At MHI, delivery is a clinical decision — because the same hormone, administered through different routes, behaves very differently inside the body.
Injectable testosterone is the gold standard for control. Carrier oil matters more than most clinics acknowledge. Cottonseed oil — the default in many commercial formulations — is the most reactive. Switching to MCT oil eliminated edema, injection site irritation, and inflammatory complaints in the overwhelming majority of our patients.
Ester selection determines release speed. Matching the ester to the individual and to the dosing frequency produces stable levels instead of peaks and crashes. The classic “rollercoaster” experience most men describe on TRT is not inevitable — it is a protocol design problem.
Pellets are the most aggressively marketed option in the industry. They are also the least controllable. Once inserted, dosing cannot be adjusted. If the amount is wrong, the patient waits months. In men, where precision matters most, most experienced clinicians avoid them entirely. A significant portion of our new patients arrive after poor pellet experiences.
If your clinic ignores the carrier oil, ignores the ester, and hands every patient the same protocol — you are not being optimized. You are being standardized.
Common signals worth measuring
These symptoms do not prove you need TRT. They mean your system deserves a real evaluation.
Physical
- Low energy
- Belly fat
- Poor recovery
- Declining strength
- Disrupted sleep
Cognitive
- Brain fog
- Low motivation
- Weak focus
- Poor resilience
Sexual & Emotional
- Diminished drive
- Low libido
- Weaker erections
- Fewer morning erections
- Mood shifts
- Loss of confidence
Most TRT clinics sell testosterone. MHI interprets male biology.
Data First
A clear biological picture before anything else. Not a quick prescription.
Interpretation Second
Labs are only meaningful when read in context. A number without clinical interpretation is noise.
Full Axis Evaluation
We assess the complete hormonal cascade — testosterone, free testosterone, SHBG, estradiol, pregnenolone, DHEA, LH, FSH, thyroid, metabolic markers, and inflammatory patterns.
Foundation Before Force
Sleep, nutrition, inflammation, stress, and metabolic health all shape how hormones behave. We address the terrain before layering tools.
Precision Protocol
Ester selection, carrier oil, delivery method, dosing frequency — every variable is chosen for your physiology, not convenience.
Ongoing Adjustment
Hormones are dynamic. Protocols are monitored and refined continuously as the system changes.
What we look at before building the plan
Hormone Axis
Total testosterone, free testosterone, SHBG, estradiol, LH, FSH, DHEA-S, pregnenolone, prolactin when indicated
Metabolic Terrain
Fasting glucose, insulin, body composition, lipid panel, liver enzymes, thyroid function
Inflammation & Risk
Cardiovascular, vascular, and systemic inflammatory markers
Fertility & Safety
Reproductive goals, PSA when appropriate, hematocrit, therapy risk planning
Recovery Inputs
Sleep quality, training load, nutrient status, cortisol patterns, and lifestyle signals shaping the system
For the man who knows something is off.
For the man who has built everything — and can feel himself running it on less.
The founder who is still executing at a high level, but knows he is forcing output that used to come naturally.
The CEO who has optimized his business down to the last variable, but has never applied that same standard to his own biology.
The high performer who is already spending serious money on health — the trainers, the supplements, the gadgets — but still does not have a coherent strategy.
The man who has been told his labs are normal, while his board, his team, and his family are getting a version of him that is operating below what he knows he is capable of.
The patient who has tried TRT before and never felt quite right — because the protocol was built for the average man, not for someone who has never accepted average in any other area of his life.
Frequently Asked Questions
There is no universal number. The value matters, but so does how you feel, your free testosterone, SHBG, estrogen balance, upstream precursors, age, goals, and risk profile. Numbers without context are just data points.
Men's Health Optimization Team
Meet the team focused on men's hormone optimization, performance, and long-term health outcomes.

Shan Siddiqi
Medical Provider

Will Alvarez
Medical Provider

Justin Latino
Medical Provider

Daniel Sanz
Wellness Optimization Specialist & Coach

Janik Brisbane
Wellness Optimization Specialist & Coach

Moe Martinez
Wellness Optimization Specialist & Coach

Tommy Fenech
Wellness Optimization Specialist & Coach
Stop guessing with your biology.
Low energy, low drive, poor recovery, brain fog, body composition changes, and declining sexual function are not character flaws. They are data. TRT may be part of the answer. Or the answer may start somewhere else entirely. But you will not know until the system is measured, interpreted, and addressed correctly.
MHI services are not covered by health insurance.